
I find it telling that I made a observation about people not believing in science when it doesn't fit their preferences and multiple posts seemed to think that was somehow politically pointed.
Did Sweden end up taking the best approach?
378,954 Views |
1675 Replies |
Last: 2 yr ago by Enzomatic
Explain policies end up being wrong? I mean, how are you going to quantify that? With models.
The "growing sense" of pessimism is based off of... what, exactly?
The numbers are not difficult. Percent infected, times percent fatality, times population. Anyone can do this math. Population is probably widely agreed.
Percent infected? Likely north of 50%, no new evidence is pushing the transmission rate down (if anything it is going up - if we take the Stanford study at face value eventual infection will be quite high).
And percent fatality. Well, this is the whole ballgame here. And nothing new has been learned since early March when we settled on a 0.5-1% range. The only thing to narrow this (or disprove it) is serology testing, and we have barely begun getting results on that.
Seeing as no new information has come in, the growing sense is basically only due to lack of what most people would consider affirming experience. As in - "I don't see people dying in my city." But that's silly, they didn't see people dying in their city a month ago. It's not new information, it's driven by a lack of understanding of what to expect. The biggest problem we have is a lack of straight talk from leadership about what to expect.
PS Epidemic modeling is not a new field. That's why I think it's pretty likely the unmitigated models that most people handwave away probably have the highest predictive value. From there, things get shaky because you're modeling human behavior.
The "growing sense" of pessimism is based off of... what, exactly?
The numbers are not difficult. Percent infected, times percent fatality, times population. Anyone can do this math. Population is probably widely agreed.
Percent infected? Likely north of 50%, no new evidence is pushing the transmission rate down (if anything it is going up - if we take the Stanford study at face value eventual infection will be quite high).
And percent fatality. Well, this is the whole ballgame here. And nothing new has been learned since early March when we settled on a 0.5-1% range. The only thing to narrow this (or disprove it) is serology testing, and we have barely begun getting results on that.
Seeing as no new information has come in, the growing sense is basically only due to lack of what most people would consider affirming experience. As in - "I don't see people dying in my city." But that's silly, they didn't see people dying in their city a month ago. It's not new information, it's driven by a lack of understanding of what to expect. The biggest problem we have is a lack of straight talk from leadership about what to expect.
PS Epidemic modeling is not a new field. That's why I think it's pretty likely the unmitigated models that most people handwave away probably have the highest predictive value. From there, things get shaky because you're modeling human behavior.
The models alone didn't drive public policy. Experts from around the world, including our own CDC and infectious disease experts were telling our leaders:
The models tried to take what we did know about the virus at the time and other similar viruses to project what the time scale of the increase would be and what different mitigation methods would yield. The CDC presented 4 scenarios to the White House. In a "do nothing scenario" it was 1.7MM deaths. In a shelter at home scenario it was 200K deaths. There were two cases in between. This information at the time was presented not to make a prediction, but to show the range of outcomes and what the sensitivity to different public policies on the outcomes was.
Clearly we have more information today than we had back then. But still, the initial assumptions still stand up. This is still a novel virus with no known vaccine, proven treatment, or cure. We have some promising ideas on treatments but clearly our daily death toll shows that nothing we have is close to a knock out punch. We see now that this is a very contagious disease that spreads exponentially through a population until a shelter at home order was put into place. We had 75 confirmed cases and 1 death on March 1st. The areas that were hardest hit did have a huge surge in hospitalizations and ICU requirements. And the social distancing has succeeded in slowing down the spread and turning the curve the other way. All of this information has been corroborated by every single front line doctor that we have on this message board, completely unfiltered from media bias.
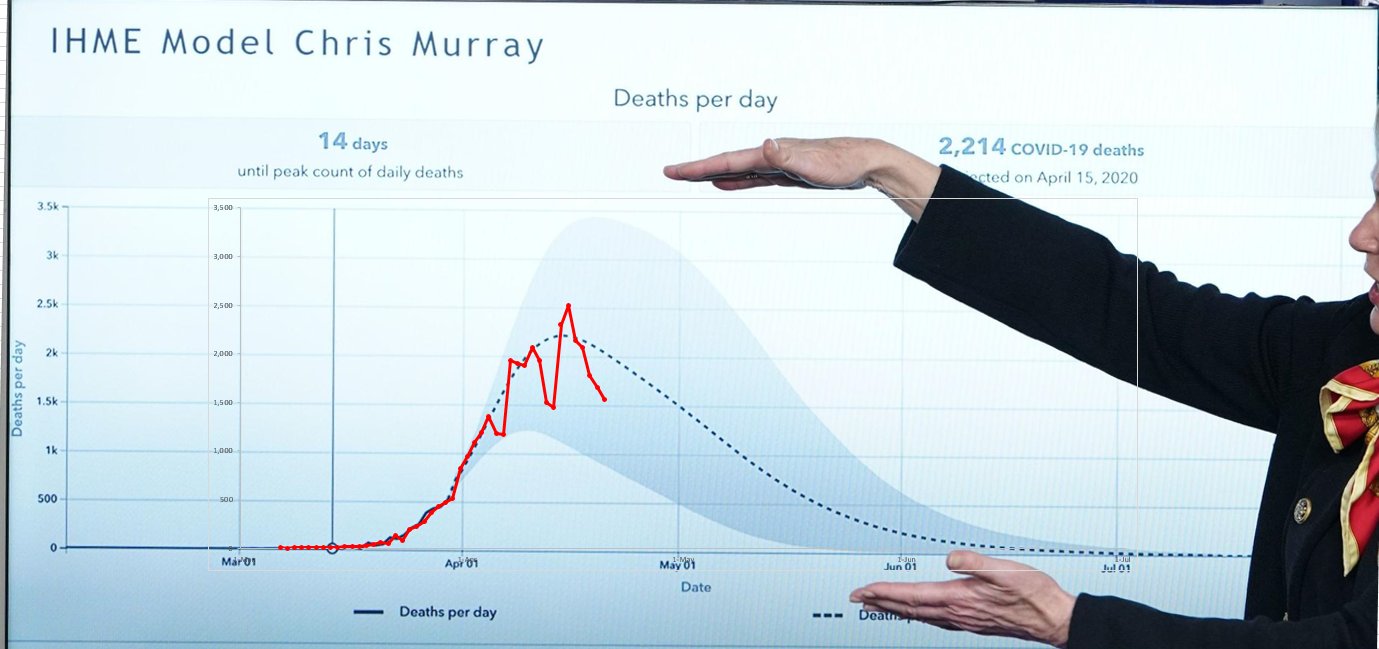
And finally, as far as the models being junk. For my own fun, I took this screen grab of a March press conference that Dr. Birx presented a version of the IHME model to talk about how many people could die as a result of the virus. At the time it was the first time the White House put a number to it -- something like 100,000 to 200,000 was said. I have graphed our daily death count over that model and have been surprised how well it has held up. Today I'd expect our daily death count to go up a lot from yesterday, since Tuesdays have been a catching up day in reporting and always high.
I think this perfectly sums up my position on the whole matter. I think this doesn't have to be so black and white for everyone. You can simultaneously fear the virus, be terrified of the economic ramifications of the shelter at home, and also be extremely skeptical of the government actions with regard to constraining liberty:
- This is a novel virus with no known vaccine, treatment or cure
- This is a highly contagious virus that spreads more rapidly than almost any virus before it
- The virus would rapidly spread exponentially through the population if nothing changed.
- This virus causes a fast surge in hospitalizations and ICU requirements which can overwhelm it and be turned into a crisis/triage situation, such as what was happening in Italy.
- The best way to handle such a virus is what South Korea SUCCESSFULLY did in quarantining, testing, contact tracing and tracking down cases before they spread. However, in order to do such a programme, you have to have those capabilities in place, which we did not at the time.
The models tried to take what we did know about the virus at the time and other similar viruses to project what the time scale of the increase would be and what different mitigation methods would yield. The CDC presented 4 scenarios to the White House. In a "do nothing scenario" it was 1.7MM deaths. In a shelter at home scenario it was 200K deaths. There were two cases in between. This information at the time was presented not to make a prediction, but to show the range of outcomes and what the sensitivity to different public policies on the outcomes was.
Clearly we have more information today than we had back then. But still, the initial assumptions still stand up. This is still a novel virus with no known vaccine, proven treatment, or cure. We have some promising ideas on treatments but clearly our daily death toll shows that nothing we have is close to a knock out punch. We see now that this is a very contagious disease that spreads exponentially through a population until a shelter at home order was put into place. We had 75 confirmed cases and 1 death on March 1st. The areas that were hardest hit did have a huge surge in hospitalizations and ICU requirements. And the social distancing has succeeded in slowing down the spread and turning the curve the other way. All of this information has been corroborated by every single front line doctor that we have on this message board, completely unfiltered from media bias.
And finally, as far as the models being junk. For my own fun, I took this screen grab of a March press conference that Dr. Birx presented a version of the IHME model to talk about how many people could die as a result of the virus. At the time it was the first time the White House put a number to it -- something like 100,000 to 200,000 was said. I have graphed our daily death count over that model and have been surprised how well it has held up. Today I'd expect our daily death count to go up a lot from yesterday, since Tuesdays have been a catching up day in reporting and always high.
I think this perfectly sums up my position on the whole matter. I think this doesn't have to be so black and white for everyone. You can simultaneously fear the virus, be terrified of the economic ramifications of the shelter at home, and also be extremely skeptical of the government actions with regard to constraining liberty:
great post
first pic is broken link though
first pic is broken link though
Are you saying we're headed towards 50% likely infected or you think/have read that we're there already?k2aggie07 said:
Percent infected? Likely north of 50%, no new evidence is pushing the transmission rate down (if anything it is going up - if we take the Stanford study at face value eventual infection will be quite high).
Do you know when in March this presser was?
I think it was March 23.
Depending on people infected, that is a huge difference in deaths. And it is beginning to look like it will be < .5%. The difference in .3-.2% and 1% is the difference in shutting down the economy and not doing so. That model is utterly useless.k2aggie07 said:
Explain policies end up being wrong? I mean, how are you going to quantify that? With models.
The "growing sense" of pessimism is based off of... what, exactly?
The numbers are not difficult. Percent infected, times percent fatality, times population. Anyone can do this math. Population is probably widely agreed.
Percent infected? Likely north of 50%, no new evidence is pushing the transmission rate down (if anything it is going up - if we take the Stanford study at face value eventual infection will be quite high).
And percent fatality. Well, this is the whole ballgame here. And nothing new has been learned since early March when we settled on a 0.5-1% range. The only thing to narrow this (or disprove it) is serology testing, and we have barely begun getting results on that.
Seeing as no new information has come in, the growing sense is basically only due to lack of what most people would consider affirming experience. As in - "I don't see people dying in my city." But that's silly, they didn't see people dying in their city a month ago. It's not new information, it's driven by a lack of understanding of what to expect. The biggest problem we have is a lack of straight talk from leadership about what to expect.
PS Epidemic modeling is not a new field. That's why I think it's pretty likely the unmitigated models that most people handwave away probably have the highest predictive value. From there, things get shaky because you're modeling human behavior.
We'll get there eventually, over ?? months (6? 12? 18??)
This is my point. Beginning to look like <0.5% based on what?
That model is useless - what model?
That model is useless - what model?
its way too early to say any policies on COVID have been wrong. that is NOT what i said.k2aggie07 said:
Explain policies end up being wrong? I mean, how are you going to quantify that? With models.
The "growing sense" of pessimism is based off of... what, exactly?
The numbers are not difficult. Percent infected, times percent fatality, times population. Anyone can do this math. Population is probably widely agreed.
Percent infected? Likely north of 50%, no new evidence is pushing the transmission rate down (if anything it is going up - if we take the Stanford study at face value eventual infection will be quite high).
And percent fatality. Well, this is the whole ballgame here. And nothing new has been learned since early March when we settled on a 0.5-1% range. The only thing to narrow this (or disprove it) is serology testing, and we have barely begun getting results on that.
Seeing as no new information has come in, the growing sense is basically only due to lack of what most people would consider affirming experience. As in - "I don't see people dying in my city." But that's silly, they didn't see people dying in their city a month ago. It's not new information, it's driven by a lack of understanding of what to expect. The biggest problem we have is a lack of straight talk from leadership about what to expect.
PS Epidemic modeling is not a new field. That's why I think it's pretty likely the unmitigated models that most people handwave away probably have the highest predictive value. From there, things get shaky because you're modeling human behavior.
i used finance in 2008 as an example - and it was quantified by markets reacting to over-leverage and securitized high risk debt bundles that models indicated were financially sound.
my point is not to judge COVID, but to make the point that public reaction if models prove wrong in this case will be extreme and detrimental to other applications of modeling in public policy.
i've re-read what I posted and think I was very clear.
We're from North California, and South Alabam
and little towns all around this land...
and little towns all around this land...
for the record i never said the 'models were junk'.
its truly a tossup who is worse - the 'panic driven defenders of shut down policy no matter what' or the 'nothing to see here open it all up' crowd.
you can't have a discussion without one camp or the other jamming you into their tantrum reaction.
its truly a tossup who is worse - the 'panic driven defenders of shut down policy no matter what' or the 'nothing to see here open it all up' crowd.
you can't have a discussion without one camp or the other jamming you into their tantrum reaction.
We're from North California, and South Alabam
and little towns all around this land...
and little towns all around this land...
I wasn't clear enough, sorry. My point is we're not going to have direct measurement to determine severity for this. Any post facto analysis will be model driven as well. That puts you in a bind of using models to show why using models is bad.
And you kinda missed the point of what I was saying. What is driving the growing sense you describe? It's certainly not data driven, as far as I can see.
And you kinda missed the point of what I was saying. What is driving the growing sense you describe? It's certainly not data driven, as far as I can see.
Thanks, that's what I thought you were saying, I just wanted to be sure.k2aggie07 said:
We'll get there eventually, over ?? months (6? 12? 18??)
we've had a steady drip of antibody testing results over the past several days that, while not remotely sufficient to draw conclusions yet, are certainly 'new information' that has come in. these tests are consistently indicating vastly larger infection rates, which significantly reduces the death rate, which significantly impacts the modeling assumptions and projections. i don't know of a single antibody result to date that indicates an infection rate in the same order of magnitude as the early model assumptions.k2aggie07 said:
Seeing as no new information has come in, the growing sense is basically only due to lack of what most people would consider affirming experience.
with regard to the epidemiological models, basic contact simulation, R0 based modeling is not new. the human behavior aspect, continuous incorporation of large data sets, and the nonlinear effects on infection rates and projections of hospitalization/death is increasingly sophisticated and prone to error.
models certainly drove public policy. best example, for better or worse, is the UK. IC model projection drove a complete shift in public policy in the UK from the Swedish approach to the shut down approach. That's a matter of public record.
To be clear: it is (in my opinion) too early to say the COVID models were wrong or drove bad policy. My comments pertain to the hypothetical discussion that, in the event the models were off mark by the level of significance the early antibody tests indicate, public confidence in scientific modeling will take a very large hit.
We're from North California, and South Alabam
and little towns all around this land...
and little towns all around this land...
k2aggie07 said:
This is my point. Beginning to look like <0.5% based on what?
That model is useless - what model?
The fact that I see people interacting everywhere and Texas is at 500 deaths out of 30 million. The fact that every time we see a revision in models it revises the IFR downward. I do believe the virus is contagious, just not very deadly, especially to non-olds and non-fats.
I have spent my entire adult life evaluating the credibility of criminals, liars, and government employees. Sometimes all 3. I can smell BS a mile away. This shutdown is a media driven hoax.
I feel strong enough that I would place a large wager that the IFR will be less than < .5% when this has burned through the population. And obviously I am not concerned for my physical safety or the physical safety of my immediate family from this virus.
Unfortunately there's been only one actual paper released about antibody testing as far as I can find, but I very well could be missing some. If you have links to any, I very much would like to read them. The one paper has some potentially serious issues.
We have a handful of press releases about results, but no papers, and none are using an FDA approved test kit. The USC and Stanford trials are being done by an overlapping team (USC doc worked on the Stanford paper) using the same Chinese manufactured kit. That kit has sensitivity and specificity measurements all over the map, (63.7-92.7% and 87%-99.5% respectively). So who knows what to make of both of those studies.
Media reports are not evidence, and they're also not models. That's the whole problem. We live in an era of fake news, rapidly disseminated information (often false), and widespread pandemic of the Dunning-Kruger effect.
The IC model is pretty interesting, as it said for total deaths with an R0 of 2.6, the range of predicted fatalities was 12,000 to 48,000 over a two year period. UK is at 17,337 right now. On what basis can we say this model was pessimistic?
We have a handful of press releases about results, but no papers, and none are using an FDA approved test kit. The USC and Stanford trials are being done by an overlapping team (USC doc worked on the Stanford paper) using the same Chinese manufactured kit. That kit has sensitivity and specificity measurements all over the map, (63.7-92.7% and 87%-99.5% respectively). So who knows what to make of both of those studies.
Media reports are not evidence, and they're also not models. That's the whole problem. We live in an era of fake news, rapidly disseminated information (often false), and widespread pandemic of the Dunning-Kruger effect.
The IC model is pretty interesting, as it said for total deaths with an R0 of 2.6, the range of predicted fatalities was 12,000 to 48,000 over a two year period. UK is at 17,337 right now. On what basis can we say this model was pessimistic?
I don't trust my gut on this. And frankly, I don't trust yours either.
its not just modelers who may face some public backlash as reality emerges...
HCQ early study
Hotard07 the most accurate thing about your venn diagram is the small size of the center of the debate.
a key question is how, in this age of instant information and social media, to grow the center.
HCQ early study
Hotard07 the most accurate thing about your venn diagram is the small size of the center of the debate.
a key question is how, in this age of instant information and social media, to grow the center.
We're from North California, and South Alabam
and little towns all around this land...
and little towns all around this land...
You can't unless you have a way to cut through selection bias. The only way I can see is for a nonpolarizing leader to emerge who can deliver straight talk to people and not ruffle feathers on either side of the political aisle. In other words, a unicorn. Probably not going to happen.
i'm referencing that original model (2M US, 500K UK) that caused so much policy shift. the later models incorporated human behavior changes and the most recent revs appear pretty accurate. its not clear that, had this current projection been originally used, policy would not have been nearly so restrictive.k2aggie07 said:
Unfortunately there's been only one actual paper released about antibody testing as far as I can find, but I very well could be missing some. If you have links to any, I very much would like to read them. The one paper has some potentially serious issues.
We have a handful of press releases about results, but no papers, and none are using an FDA approved test kit. The USC and Stanford trials are being done by an overlapping team (USC doc worked on the Stanford paper) using the same Chinese manufactured kit. That kit has sensitivity and specificity measurements all over the map, (63.7-92.7% and 87%-99.5% respectively). So who knows what to make of both of those studies.
Media reports are not evidence, and they're also not models. That's the whole problem. We live in an era of fake news, rapidly disseminated information (often false), and widespread pandemic of the Dunning-Kruger effect.
The IC model is pretty interesting, as it said for total deaths with an R0 of 2.6, the range of predicted fatalities was 12,000 to 48,000 over a two year period. UK is at 17,337 right now. On what basis can we say this model was pessimistic?
that's the point the Swede was making in the interview, i think.
i'll google links to recent public announcements of antibody tests, most recent is the USC test.
USC & Stanford
Chelsea
Teddy Roosevelt
none of it is peer reviewed (closest to peer review is the Stanford study of Santa Clara county that was still in review, if i recall), so too early to make any conclusions.
We're from North California, and South Alabam
and little towns all around this land...
and little towns all around this land...
k2aggie07 said:
I don't trust my gut on this. And frankly, I don't trust yours either.
Ok. How about a cold, hard, cost/benefit analysis hypo?
The currently projected Texas COVID deaths around 1,000.
This is obviously hyperbole, but it would have been better to keep the economy open even if that required letting DPS Troopers shoot 1,000 Texans at random on traffic stops rather than to shut down the Texas economy for. months. That gives me or any other Texan about a 1 in 30,000 chance of being shot by a Trooper or me a 50% chance of a multi-month shutdown killing my business (And I assume based on unemployment and PPP claims that over 50% of Texans face economic destruction based on a multi-month shutdown). Bring on the death Troopers.
The choice with COVID is no different. And the bottom line is that while I do not understand exponential math, you do not know the denominator. And by the time you do know, the economic devastation is a fait accompli.
You cannot in good conscience hold 30 million Texans hostage to save a few thousand. Time for Texans to be given the opportunity to take some good old fashioned risk my friend. If others are scared and/or not effected economically, then just continue to stay home. The Texas hospitals will not be overwhelmed, which was the idiotic calculation that this shutdown was based on in the first place.
I will give my Mayor and County Judge props, they never gave into the fear mongering and issued a SIP order. I can't say the same for the Governor.
We're getting into the part of the argument that a lot of us predicted weeks ago.
If the mortality numbers are lower than projected, people will complain about sheltering in place rather than realizing that sheltering in place is a large part of why the mortality numbers are lower than expected.
If the mortality numbers are lower than projected, people will complain about sheltering in place rather than realizing that sheltering in place is a large part of why the mortality numbers are lower than expected.
You do realize it's 1,000 with a large amount of social distancing?
Yet the mortality numbers are right in line with what was expected, <70yo COVID is not an issue, Nothing to fear.fig96 said:
We're getting into the part of the argument that a lot of us predicted weeks ago.
If the mortality numbers are lower than projected, people will complain about sheltering in place rather than realizing that sheltering in place is a large part of why the mortality numbers are lower than expected.
So am I. That's the point, there is a persistent misunderstanding about this. The model never changed. There was no later model. The original 2M / 500k was a baseline, and in the original paper was taken as unlikely because it didn't assume for spontaneous response. The original model is intact, is what is being used, and wasn't revised. Here, read it - note the date.Quote:
i'm referencing that original model (2M US, 500K UK) that caused so much policy shift. the later models incorporated human behavior changes and the most recent revs appear pretty accurate. its not clear that, had this current projection been originally used, policy would not have been nearly so restrictive.
The hooplah pushback and accusation that it was "revised down" started with Alex Berenson's twitter account and blew up. The lead author (Ferguson) actually had to take to twitter to clear the score. Didn't work, lie was shouted, retraction whispered.
There's only been one paper for antibody testing, and thats the Stanford one. USC and Chelsea haven't been published - no error bars, no test info. The TR was PCR, and is incredibly useful - but this isn't new. 56% asymptomatic is a far cry from what Stanford is saying which is 98%+ (50x reported)!
Trump made this argument very clearly yesterday (his last question) when he projected hundreds of thousands or millions of deaths would have resulted had we not locked down.fig96 said:
We're getting into the part of the argument that a lot of us predicted weeks ago.
If the mortality numbers are lower than projected, people will complain about sheltering in place rather than realizing that sheltering in place is a large part of why the mortality numbers are lower than expected.
its why Sweden is such a hugely important case study - the final death toll vs actual infection rate there will be the only comparative out there of an alternative approach.
I think its why there's so much passion for and against their policy - because the rest of the world uniformly went the other way, without Sweden there can't be a comparative.
of all the countries i would have guessed would defy the rest of the world, for some reason Sweden wasn't one of them.
what is happening in Singapore right now may also be comparative. surging infection rates after it appeared to be under control are worrisome.
We're from North California, and South Alabam
and little towns all around this land...
and little towns all around this land...
Ok. Let say 10,000 deaths. Than gives me a 1 in 3,000 chance. I'm still risking it. 30,000 deaths? So 1 in 1,000. Guess what? I'm still risking it.HouAggie2007 said:
You do realize it's 1,000 with a large amount of social distancing?
Texans should be given the the chance to make their own cost/benefit calculation and then the individual choice to risk it or not. Period.
i understand your point and that the baseline IC model assumptions were modified to incorporate social distancing following the policy changes (the model assumptions were changed, if that is better terminology - sorry to be pedantic but a model with different assumptions incorporated mathematically into its parameters is a different model).k2aggie07 said:So am I. That's the point, there is a persistent misunderstanding about this. The model never changed. There was no later model. The original 2M / 500k was a baseline, and in the original paper was taken as unlikely because it didn't assume for spontaneous response. The original model is intact, is what is being used, and wasn't revised. Here, read it - note the date.Quote:
i'm referencing that original model (2M US, 500K UK) that caused so much policy shift. the later models incorporated human behavior changes and the most recent revs appear pretty accurate. its not clear that, had this current projection been originally used, policy would not have been nearly so restrictive.
The hooplah pushback and accusation that it was "revised down" started with Alex Berenson's twitter account and blew up. The lead author (Ferguson) actually had to take to twitter to clear the score. Didn't work, lie was shouted, retraction whispered.
There's only been one paper for antibody testing, and thats the Stanford one. USC and Chelsea haven't been published - no error bars, no test info. The TR was PCR, and is incredibly useful - but this isn't new. 56% asymptomatic is a far cry from what Stanford is saying which is 98%+ (50x reported)!
his initial baseline projections resulted in a massive shift in policy in the UK (definitely) and the USA (I believe). we'll never know if his baseline would have proven correct (thank God) because behavior was modified. POTUS certainly believes firmly that behavior modification has saved hundreds of thousands of lives in the USA at minimum.
Sweden has modified behavior, just not through directive shut down, so any comparative will be between directive aggressive lock down and the Swedish approach. both incorporate significant behavior shift from the baseline Ferguson assumptions.
we agree regarding the antibody studies - they are very premature and as stated do not support conclusions as yet. i believe they are indicative of underestimation of infection rate, but it is too early to conclude anything.
We're from North California, and South Alabam
and little towns all around this land...
and little towns all around this land...
Player To Be Named Later

Joined:
Sep 22, 2003
Posts:
23,205
How long do you want to ignore this user?
AG
I wish it were that black and white. The problem with that line of thinking is that people who just don't care one bit and are going to behave as if nothing was going on could quite conceivably cause problems for people who are trying to be cautious by becoming spreaders.The_Fox said:Ok. Let say 10,000 deaths. Than gives me a 1 in 3,000 chance. I'm still risking it. 30,000 deaths? So 1 in 1,000. Guess what? I'm still risking it.HouAggie2007 said:
You do realize it's 1,000 with a large amount of social distancing?
Texans should be given the the chance to make their own cost/benefit calculation and then the individual choice to risk it or not. Period.
Unless you think it's 100% black and white and anyone who wants to be cautious just shouldn't come out of their homes at all.
If I were 100% confident that the only people who would be affected by carrying on as normal were the ones carrying on as normal, then I'd be completely ok with wishing you the best of luck.
No, this is incorrect. The original paper took a baseline and studied the effect of intervention against the baseline. The model assumptions were not changed. There was no modification. There was no first or second publication. Just the one.Quote:
i understand your point and that the baseline IC model assumptions were modified to incorporate social distancing following the policy changes (the model assumptions were changed, if that is better terminology - sorry to be pedantic but a model with different assumptions incorporated mathematically into its parameters is a different model).
Yes. Next question.Player To Be Named Later said:I wish it were that black and white. The problem with that line of thinking is that people who just don't care one bit and are going to behave as if nothing was going on could quite conceivably cause problems for people who are trying to be cautious by becoming spreaders.The_Fox said:Ok. Let say 10,000 deaths. Than gives me a 1 in 3,000 chance. I'm still risking it. 30,000 deaths? So 1 in 1,000. Guess what? I'm still risking it.HouAggie2007 said:
You do realize it's 1,000 with a large amount of social distancing?
Texans should be given the the chance to make their own cost/benefit calculation and then the individual choice to risk it or not. Period.
Unless you think it's 100% black and white and anyone who wants to be cautious just shouldn't come out of their homes at all.
If I were 100% confident that the only people who would be affected by carrying on as normal were the ones carrying on as normal, then I'd be completely ok with wishing you the best of luck.
I quit listening to the pressers a few weeks back so I'll take your word for it 
But you're right, Sweden is definitely the outlier and an interesting case study in all this I think in order to really compare we'll need to evaluate how different what they were doing actually was vs how society lent itself to that (high speed internet, lots of tech that easily works remotely, large single population, voluntary social distancing) and that's going to be tougher to quantify.
But you're right, Sweden is definitely the outlier and an interesting case study in all this I think in order to really compare we'll need to evaluate how different what they were doing actually was vs how society lent itself to that (high speed internet, lots of tech that easily works remotely, large single population, voluntary social distancing) and that's going to be tougher to quantify.
People use this, along with "Americans are selfish and won't change naturally in response to a deadly pathogen" as strawmen.fig96 said:
I quit listening to the pressers a few weeks back so I'll take your word for it
But you're right, Sweden is definitely the outlier and an interesting case study in all this I think in order to really compare we'll need to evaluate how different what they were doing actually was vs how society lent itself to that (high speed internet, lots of tech that easily works remotely, large single population, voluntary social distancing) and that's going to be tougher to quantify.
Thankfully American cities are unique and isolated enough to confidently make this comparison. Silicon valley very much fits that description, and they had the hardest and earliest lockdown in the US. As such, we can gain much when this is all over between the Swedish model and SV, for example.
Mike Shaw - Class of '03
How is it a strawman?NASAg03 said:People use this, along with "Americans are selfish and won't change naturally in response to a deadly pathogen" as strawmen.fig96 said:
I quit listening to the pressers a few weeks back so I'll take your word for it
But you're right, Sweden is definitely the outlier and an interesting case study in all this I think in order to really compare we'll need to evaluate how different what they were doing actually was vs how society lent itself to that (high speed internet, lots of tech that easily works remotely, large single population, voluntary social distancing) and that's going to be tougher to quantify.
Thankfully American cities are unique and isolated enough to confidently make this comparison. Silicon valley very much fits that description, and they had the hardest and earliest lockdown in the US. As such, we can gain much when this is all over between the Swedish model and SV, for example.
I'm not saying not to use it or that it isn't relevant, just that it needs to be evaluated in context (which is something people tend not to do).
Featured Stories
See All
Cashius Howell validated and vindicated by postseason honors
by Olin Buchanan
Cashius Howell and Trey Zuhn III among 2025 SEC Award winners
by Richard Zane
Bobby Shuttleworth hired as Texas A&M's next head soccer coach
by Richard Zane
24:24
10h ago
7.3k
7:32
7h ago
2.4k