
This is a success story thread. You can go start your own thread if you wish.
HCQ (cocktail) Success Stories
35,603 Views |
278 Replies |
Last: 5 yr ago by jagvocate
Doctors Worldwide Rate Hydroxychloroquine Most Effective Therapy for Coronavirus Infection
https://www.precisionvaccinations.com/fda-issued-emergency-authorization-hydroxychloroquine-treatment-covid-19-patients-usa
https://www.precisionvaccinations.com/fda-issued-emergency-authorization-hydroxychloroquine-treatment-covid-19-patients-usa
Quote:
A global survey found that anti-malarial drug hydroxychloroquine was the most highly-rated treatment against the coronavirus disease 2019 (COVID-19).
This new survey completed by Sermo on March 27, 2020, reported 6,227 physicians in 30 countries found that 37 percent of those treating COVID-19 patients rated hydroxychloroquine as the "most effective therapy" from a list of 15 options.
Below is a summary of the findings from the Sermo survey:
- Hydroxychloroquine usage amongst COVID-19 treaters is 72% in Spain, 49% in Italy, 41% in Brazil, 39% in Mexico, 28% in France, 23% in the US, 17% in Germany, 16% in Canada, 13% in the UK and 7% in Japan.
- Hydroxychloroquine was overall chosen as the most effective therapy from a list of 15 options (37% of COVID-19 treaters).
- 75% in Spain, 53% in Italy, 44% in China, 43% in Brazil, 29% in France, 23% in the US and 13% in the UK.
- The two most common treatment regimens for Hydroxychloroquine were: (38%) 400mg twice daily on day one; 400 mg daily for 5 days. (26%) 400mg twice daily on day one; 200mg twice daily for 4 days.
- Outside the US, Hydroxychloroquine was equally used for diagnosed patients with mild to severe symptoms whereas in the US it was most commonly used for high risk diagnosed patients.
- Globally, 19% of physicians prescribed or have seen Hydroxychloroquine prophylactically used for high-risk patients, and 8% for low-risk patients.
Iceland has been using Hydroxychloroquine for Covid-19 Since Early April, 2020: Shipment of Antimalarial Drug Has Arrived
https://icelandmonitor.mbl.is/news/news/2020/04/07/shipment_of_antimalarial_drug_has_arrived/
Quote:
The kinds of drugs thought to be the likeliest to be effective against the coronavirus are Chloroquine and Hydroxychloroquine; the drug Kaletra, which is used for the treatment and prevention of HIV/AIDS; and Remdesivir, which was developed by Gilead Sciences as a treatment for Ebola virus disease. India is the largest manufacturer of Hydroxychloroquine, the export of which the country has now banned, so that it can be used within their borders. Alvogen feared a ban would be imposed on the export of Chloroquine as well, making the drug next to impossible to access
An E.R. Doctor Infected With Covid-19 Back At Work After Using Hydroxychloroquine and Z-Pak Protocol
India: Govt expands Hydroxychloroquine as prophylactic for healthcare workers
https://www.livemint.com/politics/policy/govt-expands-hydroxychloroquine-as-prophylactic-for-healthcare-workers-11590170414019.html
This thread is NOT intended to spark political debate. It is only to show what works and hopefully be a resource and save lives. In fact, if you have a case where the drug worked using the 3 way cocktail, please post. No political opinions please.
https://www.livemint.com/politics/policy/govt-expands-hydroxychloroquine-as-prophylactic-for-healthcare-workers-11590170414019.html
Quote:
NEW DELHI : After some promising results on the efficacy of prophylactic use of Hydroxychloroquine (HCQ) against COVID-19 infection, the Central government has expanded the use of the medicine as prophylaxis to healthcare and other frontline workers deployed in non-COVID and COVID area.
The Union Health Ministry on Thursday revised advisory on the use of HCQ as prophylactic for COVID-19 infection.
The decision came after the National Task Force (NTF) for COVID-19 constituted by the Indian Council of Medical Research (ICMR) reviewed the use of HCQ for prophylaxis of SARS-CoV-2 infection for high-risk population based on the emerging evidence on its safety and efficacy.
This thread is NOT intended to spark political debate. It is only to show what works and hopefully be a resource and save lives. In fact, if you have a case where the drug worked using the 3 way cocktail, please post. No political opinions please.
leading off with an article from The Gateway Pundit is not a good way to show you
1. Don't intend the thread to be political
2. Want to use fact based evidence
1. Don't intend the thread to be political
2. Want to use fact based evidence
And then, it was immediately followed up with an article entitled "Why do I have to go to African YouTube to see this" and quoted something about "Trump derangement syndrome", whatever that is.nai06 said:
leading off with an article from The Gateway Pundit is not a good way to show you
1. Don't intend the thread to be political
2. Want to use fact based evidence
You're not furthering the saving of lives by digging through some of the most blatantly political websites on the internet and posting their articles about "Critics blast[ing] Trump", "Debunking Dem myths", "Democratic state representatives" and what medicine Amy Klobuchar's husband "thinks" he took. Nor are Sharyl Atkinson and Laura Ingraham commentaries furthering the pursuit of scientific solutions.Quote:
This thread is NOT intended to spark political debate. It is only to show what works and hopefully be a resource and save lives. In fact, if you have a case where the drug worked using the 3 way cocktail, please post. No political opinions please.
To the extent there is useful information tucked in this thread (maybe the ScienceTimes article about the NYU study), its completed railroaded by that stuff and destroys any possibility the discussion will become productive.

Experts at UTHealth successfully treat severe case of COVID-19 in 3-week-old infant
https://www.eurekalert.org/pub_releases/2020-04/uoth-eau042820.php
https://www.eurekalert.org/pub_releases/2020-04/uoth-eau042820.php
Quote:
In one of the first reported cases of its kind, a 3-week-old infant in critical condition recovered from COVID-19 due to rapid recognition and treatment by physicians from McGovern Medical School at The University of Texas Health Science Center at Houston (UTHealth). The case was published April 22 in the New England Journal of Medicine.
As more data is released on COVID-19, the original belief that pediatric patients are spared from the worst of the disease has been disproven.
"We are still so early in the research and data available on COVID-19, and as providers, we need to be aware that children can get critically ill from this virus," said Alvaro Coronado Munoz, MD, first author and assistant professor of pediatric critical care medicine at McGovern Medical School at UTHealth. "It's important for parents to understand that they should not delay seeking care for their children if there's any presence of fever or trouble breathing."
The child first presented at a local hospital with nasal congestion, rapid breathing, and reduced eating. Physicians there recorded a temperature of 97.0 degrees, high pulse rate, and low oxygen saturation. The child was transferred to a pediatric intensive care unit, and Coronado and other team members were alerted. Upon arrival, the child had low blood pressure and hypothermia, as well as continued rapid heart rate and breathing. Lung X-rays revealed opacity and collapse in one of the upper lobes, indications of pneumonia.
As it was early in the pandemic, it would take a week for test results from a nasal swab to return as positive for the coronavirus, but physicians did not wait before moving into a COVID-19 action plan for the pediatric intensive care unit (PICU).
A repost of vital information; download entire pdf (17 pages with various color graphs and charts). Note the prophylaxis part can be done with over the counter supplements. Although this is written by physicians, always consult with your before taking anything.
East Virginia Medical School Medical Group EVMS Critical Care Covid-19 Management Protocol
https://www.evms.edu/media/evms_public/departments/internal_medicine/EVMS_Critical_Care_COVID-19_Protocol.pdf
There is more, recommend downloading the entire pdf (17 pages)
East Virginia Medical School Medical Group EVMS Critical Care Covid-19 Management Protocol
https://www.evms.edu/media/evms_public/departments/internal_medicine/EVMS_Critical_Care_COVID-19_Protocol.pdf
Quote:
Prophylaxis
While there is very limited data (and none specific for COVID-19), the following "cocktail" may have a role in the prevention/mitigation of COVID-19 disease. While there is no high-level evidence that this cocktail is effective; it is cheap, safe and widely available.
Vitamin C 500 mg BID and Quercetin 250-500 mg BID [1 -5] Zinc 75-100 mg/day (acetate, gluconate or picolinate). Zinc lozenges are preferred. After 1 month, reduce the dose to 30-50 mg/day. [1,6-9]
Melatonin (slow release): Begin with 0.3mg and increase as tolerated to 2 mg at night [10-13]
Vitamin D3 1000-4000 u/day [14-20]Optional: Famotidine 20-40mg/day [21]
Optional/uncertain: Once weekly chloroquine/hydroxychloroquine may have a role in prophylaxis in high risk subgroups i.e. heath care workers, residents of nursing homes, etc. Ongoing studies are testing this hypothesis.
Symptomatic patients (at home):
Vitamin C 500 mg BID and Quercetin 250-500 mg BID Zinc 75-100 mg/day
Melatonin 6-12 mg at night (the optimal dose is unknown)Vitamin D3 2000-4000 u/day
Optional: ASA 81 -325 mg/day
Optional: Famotidine 20-40mg/day
Optional: Hydroxychloroquine 400mg BID day 1 followed by 200mg BID for 4 days [22]. Recent evidence suggests that HCQ has no role in the treatment of COVID-19 in hospitalized patients.[23] However, the potential role of HCQ in early symptomatic patients (prior to hospitalization) is unknown.
Optional: Ivermectin 150-200 ug/kg (single dose) [24,25]
In symptomatic patients, monitoring with home pulse oximetry is recommended. Ambulatory desaturation < 94% should prompt hospital admission
Mildly Symptomatic patients (on floor):
Vitamin C 500 mg q 6 hourly and Quercetin 250-500 mg BID (if available)
Zinc 75-100 mg/day
Melatonin 6-12 mg at night (the optimal dose is unknown)
Vitamin D3 2000-4000 u/day
Enoxaparin 60 mg daily [26-30]
Methylprednisolone 40 mg q 12 hourly ; increase to 80 mg q 12 hourly in patients with progressive symptoms and increasing CRP. [31-35]
Famotidine 40mg daily (20 mg in renal impairment)
Optional: Remdesivir,200 mg IV loading dose D1, followed by 100mg day IV for 9 days. [36,37]This agent has been reported to reduce time to recovery (based on an ordinal scale). [37] The benefit of this agent on patient centered outcomes is unclear.
Optional: Ivermectin 150-200 ug/kg (single dose)
N/C 2L /min if required (max 4 L/min; consider early t/f to ICU for escalation of care).
Avoid Nebulization and Respiratory treatments. Use "Spinhaler" or MDI and spacer if required.
Avoid CPAP or BiPAP
T/f EARLY to the ICU for increasing respiratory signs/symptoms and arterial desaturation.
Respiratory symptoms (SOB; hypoxia- requiring N/C 4 L min: admit to ICU): Essential Treatment (dampening the STORM)
1.Methylprednisolone 80 mg loading dose then 40mg q 12 hourly for at least 7 days and until transferred out of ICU. In patients with an increasing CRP or worsening clinical status increase the dose to 80 mg q 12 hourly, then titrate down as appropriate. [31-35]
2.Ascorbic acid (Vitamin C) 3g IV q 6 hourly for at least 7 days and/or until transferred out of ICU. Note caution with POC glucose testing (see below). [38-46]
3.Full anticoagulation: Unless contraindicated we suggest FULL anticoagulation (on admission to the ICU) with enoxaparin, i.e 1 mg kg s/c q 12 hourly (dose adjust with Cr Cl < 30mls/min). [26-30]Heparin is suggested with CrCl < 15 ml/min. Alternative approach: Half-dose rTPA: 25mg of tPA over 2 hours followed by a 25mg tPA infusion administered over the subsequent 22 hours, with a dose not to exceed 0.9 mg/kg followed by full anticoagulation.
Note: A falling SaO2 despite respiratory symptoms should be a trigger to start anti-inflammatory treatment (see Figure 2).
Note: Early termination of ascorbic acid and corticosteroids will likely result in a rebound effect with clinical deterioration (see Figure 3).
Additional Treatment Components (the Full Monty)
4.Melatonin 6-12 mg at night (the optimal dose is unknown).
5.Famotidine 40mg daily (20 mg in renal impairment)
6.Vitamin D 2000-4000 u PO daily
7.Thiamine 200 mg IV q 12 hourly
8.Magnesium: 2 g stat IV. Keep Mg between 2.0 and 2.4 mmol/l. Prevent hypomagnesemia (which increases the cytokine storm and prolongs Qtc). [47-49]
9.Optional: Azithromycin 500 mg day 1 then 250 mg for 4 days (has immunomodulating properties including downregulating IL-6; in addition, Rx of concomitant bacterial pneumonia). [50]
10.Optional: Simvastatin 80 mg/day. Of theoretical but unproven benefit. Simvastatin has been demonstrated to reduce mortality in the hyper-inflammatory ARDS phenotype. [51] Statins have pleotropic anti-inflammatory, immunomodulatory, antibacterial and antiviral effects. In addition, statins decrease expression of PAI-1.
11.Optional: Remdesivir. The role of this agent in patients with more advanced pulmonary involvement appears to be limited.
12.Broad-spectrum antibiotics if superadded bacterial pneumonia is suspected based on procalcitonin levels and resp. culture (no bronchoscopy). Due to the paradox of hyper-inflammation and immune suppression (a major decrease of HLA-DR on CD14 monocytes) secondary bacterial infection is not uncommon.
13.Maintain EUVOLEMIA (this is not non-cardiogenic pulmonary edema). Due to the prolonged "symptomatic phase" with flu-like symptoms (6-8 days) patients may be volume depleted. Cautious rehydration with 500 ml boluses of Lactate Ringers may be warranted, ideally guided by non-invasive hemodynamic monitoring. Diuretics should be avoided unless the patient has obvious intravascular volume overload. Avoid hypovolemia.
14.Early norepinephrine for hypotension.
15.Escalation of respiratory support (steps); Try to avoid intubation if at all possible, (see Figure 4)
Accept "permissive hypoxemia" (keep O2 Saturation > 84%); follow venous lactate and Central Venous O2 saturations (ScvO2) in patents with low arterial O2 saturations
N/C 1-6 L/min
High Flow Nasal canula (HFNC) up to 60-80 L/min
Trial of inhaled Flolan (epoprostenol)
Attempt proning (cooperative repositioning-proning)
Intubation ... by Expert intubator; Rapid sequence. No Bagging; Full PPE. Crash/emergency intubations should be avoided.
Volume protective ventilation; Lowest driving pressure and lowest PEEP as possible. Keep driving pressures < 15 cmH2O.
Moderate sedation to prevent self-extubation
Trial of inhaled Flolan (epoprostenol)
Prone positioning.
There is widespread concern that using HFNC could increase the risk of viral transmission. There is however, no evidence to support this fear. HFNC is a better option for the patient and the health care system than intubation and mechanical ventilation. CPAP/BiPAP may be used in select patients, notably those with COPD exacerbation or heart failure. A sub-group of patients with COVID-19 deteriorates very rapidly. Intubation and mechanical ventilation may be required in these patients
16. Salvage Treatments
Plasma exchange [52-54]. Should be considered in patients with progressive oxygenation failure despite corticosteroid therapy. Patients may require up to 5 exchanges.
High dose corticosteroids; 120mg methylprednisolone q 6-8 hourly
Siltuximab and Tocilizumab (IL-6 inhibitors) [55,56]
Convalescent serum; the role and timing of convalescent serum are uncertain. [57-59]
CVVH with cytokine absorbing/filtering filters [60]
?? ECMO < 60 yrs. and no severe commodities/organ failure [61]. Unlike "typical ARDS" patients do not progress into a resolution phase. Rather, patients with COVID-19 progress to a severe fibro-proliferative phase and ventilator dependency. ECMO is these patients would serve very little purpose.
17.Treatment of Macro****e Activation Syndrome (MAS)
A sub-group of patients will develop MAS. This appears to be driven by SARS-CoV-2 induced inflammasome activation and increased IL-1 production (see Figure 5). [62,63]
A ferritin > 4400 ng/ml is considered diagnostic of MAS. Other diagnostic features include increasing AST/ALT and increasing CRP. [64]
"High dose corticosteroids." Methylprednisolone 120 mg q 6-8 hourly for at least 3 days, then wean according to Ferritin, CRP, AST/ALT (see Figure 6). Ferritin should decrease by at least 15% before weaning corticosteroids.
Consider plasma exchange.
Anakinra (competitively inhibits IL-1 binding to the interleukin-1 type I receptor) can be considered in treatment failures.
18.Monitoring
Daily: PCT, CRP, IL-6, BNP, Troponins, Ferritin, Neutrophil-Lymphocyte ratio, D-dimer and Mg. CRP, IL-6 and Ferritin track disease severity closely (although ferritin tends to lag behind CRP). Early CRP levels are closely associated with the degree of pulmonary involvement and the CT score. [65] Thromboelastogram (TEG) on admission and repeated as indicated.
In patients receiving IV vitamin C, the Accu-Chek POC glucose monitor will result in spuriously high blood glucose values. Therefore, a laboratory glucose is recommended to confirm the blood glucose levels.
Monitor QTc interval if using chloroquine/hydrochloroquine and azithromycin and monitor Mg++ (torsades is uncommon in monitored ICU patients)
No routine CT scans, follow CXR and chest ultrasound.
Follow ECHO closely; Pts develop a severe cardiomyopathy.
19.Post ICU management
a.Enoxaparin 40-60 mg s/c daily
b.Methylprednisolone 40 mg day, then wean slowly
c.Vitamin C 500 mg PO BID
d.Melatonin 3-6 mg at night
There is more, recommend downloading the entire pdf (17 pages)
Excellent work!
Honestly will we ever see a double blind controlled study on this? I seriously doubt it. Not in big pharma's interest because there is no money to be made for them at all
I am still baffled that there seem to be two groups of Doctors. One set says "good stuff" the other says "nope doesn't work".
In all seriousness a study that addresses how doctors developed their treatment protocols in the early stages of the Covid wave would be useful to understand. What factors did doctors have to weigh and consider. Where there single or multiple sources? How much was influenced when Wuhan was the epicenter? Did protocols change when models where recalibrated? There would be hundreds of questions that could be asked.
In all seriousness a study that addresses how doctors developed their treatment protocols in the early stages of the Covid wave would be useful to understand. What factors did doctors have to weigh and consider. Where there single or multiple sources? How much was influenced when Wuhan was the epicenter? Did protocols change when models where recalibrated? There would be hundreds of questions that could be asked.
From Dr. Coates,
Finally, here is a new paper out of Yale Medical School recommending the use of HCQ/zithromax or Doxycycline and Zinc as outpatient treatment.
Please note this is not a study but rather it is a paper reviewing all of the data on outpatient benefits. He feels this information needs to get out as it will likely be September before we get actual randomized control trials available on outpatient treatment. He fears too many will needlessly die in that time due to fear of using HCQ with zithromax or doxycycline due to recent statements by the FDA. So he is essentially doing a metaanalysis of the available data. He reviews many outpatient studies and the results of each. The author believes the results are far from anecdotal and goes into the pluses and minuses of each study. He also mentions many of the hospitalized studies and points out similar to I did Monday the faults of these studies. I think he does a good job going over the valid points and things that are not relevant in the quoted studies. I have included a few good quotes for those interested and you can read the study in it's entirety below.
"Available evidence of efficacy of HCQ+AZ has been repeatedly described in the media as "anecdotal," but most certainly is not. The evidence is not perfect either. "
"evidence for single agents cannot be extrapolated to apply to combined agents, evidence for one biochemical form of a drug cannot be extrapolated to another form, and even more importantly, evidence for utility or lack thereof or toxicity in hospitalized patients cannot be extrapolated to apply to outpatient use"
"In reviewing all available evidence, I will show that HCQ+AZ and HCQ+doxycycline are generally safe for short-term use in the early treatment of most symptomatic high-risk outpatients, where not contraindicated, and that they are effective in preventing hospitalization for the overwhelming majority of such patients. If these combined medications become standard-of-care, they are likely to save an enormous number of lives that would otherwise be lost to this endemic disease."
Download the PDF at the bottom of the page.
https://academic.oup.com//advance-article/doi/10.1093/aje/
Finally, here is a new paper out of Yale Medical School recommending the use of HCQ/zithromax or Doxycycline and Zinc as outpatient treatment.
Please note this is not a study but rather it is a paper reviewing all of the data on outpatient benefits. He feels this information needs to get out as it will likely be September before we get actual randomized control trials available on outpatient treatment. He fears too many will needlessly die in that time due to fear of using HCQ with zithromax or doxycycline due to recent statements by the FDA. So he is essentially doing a metaanalysis of the available data. He reviews many outpatient studies and the results of each. The author believes the results are far from anecdotal and goes into the pluses and minuses of each study. He also mentions many of the hospitalized studies and points out similar to I did Monday the faults of these studies. I think he does a good job going over the valid points and things that are not relevant in the quoted studies. I have included a few good quotes for those interested and you can read the study in it's entirety below.
"Available evidence of efficacy of HCQ+AZ has been repeatedly described in the media as "anecdotal," but most certainly is not. The evidence is not perfect either. "
"evidence for single agents cannot be extrapolated to apply to combined agents, evidence for one biochemical form of a drug cannot be extrapolated to another form, and even more importantly, evidence for utility or lack thereof or toxicity in hospitalized patients cannot be extrapolated to apply to outpatient use"
"In reviewing all available evidence, I will show that HCQ+AZ and HCQ+doxycycline are generally safe for short-term use in the early treatment of most symptomatic high-risk outpatients, where not contraindicated, and that they are effective in preventing hospitalization for the overwhelming majority of such patients. If these combined medications become standard-of-care, they are likely to save an enormous number of lives that would otherwise be lost to this endemic disease."
Download the PDF at the bottom of the page.
https://academic.oup.com//advance-article/doi/10.1093/aje/
Yale paper finds strong evidence for efficacy of use of hydroxychloroquine and azithromycin as COVID treatment
https://video.foxnews.com/v/6160199007001#sp=show-clips
https://video.foxnews.com/v/6160199007001#sp=show-clips
Hydroxychloroquine Results That Further Vindicate Trump
https://trendingpolitics.com/breaking-la-doctor-vindicates-trump-over-hydroxychloroquine-after-seeing-breakthrough-results/
https://trendingpolitics.com/breaking-la-doctor-vindicates-trump-over-hydroxychloroquine-after-seeing-breakthrough-results/
Quote:
"Every patient I've prescribed it to has been very, very ill and within 8 to 12 hours, they were basically symptom-free," Cardillo told Eyewitness News. "So clinically I am seeing a resolution."
Rep. Mike Kelly explains why he took hydroxychloroquine while battling coronavirus
https://www.weny.com/story/42181158/rep-mike-kelly-explains-why-he-took-hydroxychloroquine-while-battling-coronavirus
https://www.weny.com/story/42181158/rep-mike-kelly-explains-why-he-took-hydroxychloroquine-while-battling-coronavirus
Quote:
Kelly tells WENY News plenty of personal research and discussions with his doctor guided his decision to take hydroxychloroquine.
"He said 'okay, I can't tell you you're right and I can't tell you you're wrong'," Kelly recalled of the conversation between he and his doctor. "'I can just tell you that you've looked at it pretty strongly and I would concur with you that your general state of health, you're a pretty good candidate for this.' So, I started taking it."
The prescription was relatively short.
"A total of nine pills, ten pills, one each day for that," Kelly said.
Kelly was diagnosed with COVID-19 two months ago on March 27 after he was tested at a drive-thru clinic in Butler, Pa. The 72-year-old was quarantined in his Butler home for over a month, and was officially considered coronavirus-free on May 6. He is now participating in a national clinical trial studying the effectiveness of blood transfusion for treating COVID-19.
Prestigious medical journal urges outpatient use of hydroxychloroquine regimen for COVID-19
https://justthenews.com/politics-policy/coronavirus/hydroxychloroquine-plus-azithromycin
https://justthenews.com/politics-policy/coronavirus/hydroxychloroquine-plus-azithromycin
Quote:
A prestigious medical journal is criticizing news media coverage of hydroxychlorioquine in the battle against coronavirus, saying there is evidence the anti-malarial drug combined with the antibiotic azithromycin helps in the early stages of outpatient treatment.
"These medications need to be widely available and promoted immediately for physicians to prescribe," the American Journal of Epidemiology reported in an article published this week that pushed back against claims the regimen has been dangerous or ineffective in all cases.
Orange County Doctor Cites Positive Results Using Hydroxychloroquine
https://www.theepochtimes.com/orange-county-doctor-cites-positive-results-using-hydroxychloroquine_3368643.html
https://www.theepochtimes.com/orange-county-doctor-cites-positive-results-using-hydroxychloroquine_3368643.html
Quote:
Dr. Gregg DeNicola is one of the first doctors in Southern California to develop a cohesive treatment plan for COVID-19 that includes the widely debated drug hydroxychloroquineand he told The Epoch Times he's seen only positive results.
"A couple [patients] look you in the eye and say, 'I think I'm going to die,'" DeNicola said. But none of the Laguna Beach-based doctor's 95 COVID-19 patients have died yet, and he credits hydroxychloroquine with helping to save them.
Coronavirus: How Turkey took control of Covid-19 emergency
https://www.bbc.com/news/world-europe-52831017
https://www.bbc.com/news/world-europe-52831017
Quote:
Chief doctor Nurettin Yiyit - whose art work is on the hospital walls - says it's key to use hydroxychloroquine early. "Other countries are using this drug too late," he says, "especially the United States. We only use it at the beginning. We have no hesitation about this drug. We believe it's effective because we get the results."
On a tour of the hospital, adding and subtracting protective layers as we go, he explains that Turkey's approach is to "get ahead of the virus", by treating early and treating aggressively. They use hydroxychloroquine and other drugs, along with blood plasma and oxygen in high concentrations.
VIDEO: Yale paper finds strong evidence for efficacy of use of hydroxychloroquine and azithromycin as COVID treatment
https://news.yahoo.com/yale-paper-finds-strong-evidence-031737798.html
https://news.yahoo.com/yale-paper-finds-strong-evidence-031737798.html
Treating Patients With Hydroxychloroquine
DeNicola said the controversy surrounding the drug "makes no sense." The drug has been used since the 20th century to treat connective tissue diseases, he said, and prescribing it has been "second nature" to him.
"I just can't explain all the negativity to it all I can do is report what I saw," he said, citing a 100 percent recovery rate.
DeNicola said the controversy surrounding the drug "makes no sense." The drug has been used since the 20th century to treat connective tissue diseases, he said, and prescribing it has been "second nature" to him.
"I just can't explain all the negativity to it all I can do is report what I saw," he said, citing a 100 percent recovery rate.
Looks like the Lancet study was incorrect and maybe done on purpose to mislead. Sad.
"As for the Lancet study I reviewed a week or so ago, the data they used has been called into serious question. It was found that the deaths they reported for Australia were more than then the country had at the time. When questioned about this the authors responded that they used Surgisphere to collect the data. Surgisphere reponsed saying one of the hospitals they thought was in Australia was actually in Asia. Doctors are now requesting that all of the data needs to be accounted for however they say they are unable to share that data.
Today the Lancet released an "Expression of Concern to alert readers to the fact that serious scientific questions have been brought to our attention." I think this along with all of the other points I mentioned last week really makes the conclusions of this study very questionable.
https://www.theguardian.com//questions-raised-over-hydroxy
https://www.tctmd.com//lancet-covid-19-hydroxychloroquine-
https://marlin-prod.literatumonline.com//S0140673620312903"
"As for the Lancet study I reviewed a week or so ago, the data they used has been called into serious question. It was found that the deaths they reported for Australia were more than then the country had at the time. When questioned about this the authors responded that they used Surgisphere to collect the data. Surgisphere reponsed saying one of the hospitals they thought was in Australia was actually in Asia. Doctors are now requesting that all of the data needs to be accounted for however they say they are unable to share that data.
Today the Lancet released an "Expression of Concern to alert readers to the fact that serious scientific questions have been brought to our attention." I think this along with all of the other points I mentioned last week really makes the conclusions of this study very questionable.
https://www.theguardian.com//questions-raised-over-hydroxy
https://www.tctmd.com//lancet-covid-19-hydroxychloroquine-
https://marlin-prod.literatumonline.com//S0140673620312903"
Yep. No science at all behind the study that was conducted by a sci-fi writer and an adult film star model.
https://www.theguardian.com/world/2020/jun/03/covid-19-surgisphere-who-world-health-organization-hydroxychloroquine
https://www.theguardian.com/world/2020/jun/03/covid-19-surgisphere-who-world-health-organization-hydroxychloroquine
COVID-19: Nigerian study finds Chloroquine, Hydroxychloroquine effective as Prophylaxis
https://www.vanguardngr.com/2020/06/covid-19-nigerian-study-finds-chloroquine-hydroxychloroquine-effective-as-prophylaxis/
https://www.vanguardngr.com/2020/06/covid-19-nigerian-study-finds-chloroquine-hydroxychloroquine-effective-as-prophylaxis/
Quote:
Speaking further, Bright observed that there were 100 percent positive outcome and zero deaths with 4Aminoquinolines in COVID-19 Response, stressing that quinine works in an advanced stage of COVID-19 as the case of the single laboratory tested positive clients have shown. "Although it has been proven that CQ/HCQ is effective in early COVID-19, more studies will be needed due to the small sample size deployed while quinine is effective in the advanced stage of COVID-19 including ICU "However, post-treatment intermittent prophylaxis is recommended in COVID-19. This is why mentioned earlier that more studies are needed," she said.
According to her, the LWI Study Protocols for COVID-19 Response is affordable, scalable, and replicable for all Africans and in the Diaspora. "Recently it was discovered that some tertiary health institutions are using the LWI Study Protocols for COVID-19 Prophylaxis and Outpatient Care. The reason is obvious. "Chloroquine / Hydroxychloroquine has multiple modes of action which prevents the virus from penetrating the host cell using its S protein and Protease. It breaks the polymerase chain and prevents viral replication. "It is a zinc ionophore and ensures penetration of zinc into the viral cell." She added.
For what it's worth, a popular family medicine doctor here in McKinney wrote this on the topic of HCQ and the soccess he and a colleague have experienced. It's not a statistically significant sample size but he's pretty convinced.
Sorry for the quality. I think he gave hard copies to patients with permission to share and I just grabbed it from the community FB group.

Edit:: weird emoji choice on my part.
Sorry for the quality. I think he gave hard copies to patients with permission to share and I just grabbed it from the community FB group.
Edit:: weird emoji choice on my part.
He and his colleague should publish his data instead of writing chain email letters to hand out to patients.McKinney Ag said:
For what it's worth, a popular family medicine doctor here in McKinney wrote this on the topic of HCQ and the soccess he and a colleague have experienced. It's not a statistically significant sample size but he's pretty convinced.
Sorry for the quality. I think he gave hard copies to patients with permission to share and I just grabbed it from the community FB group.
Edit:: weird emoji choice on my part.
That's a pretty unprofessional, if not just plain unhinged, letter.
I liked the letter.
Philippians 4:13
Fox News medical correspondent claims hydroxychloroquine cured his 96-year-old father of coronavirus
https://www.washingtonexaminer.com/news/wow-fox-news-medical-correspondent-claims-hydroxychloroquine-cured-his-96-year-old-father-of-coronavirus
Quote:
"Tucker, I want to tell you about a 96-year-old man in Florida who said one night, 'I don't think I'm going to make it. I feel very weak. The end is coming. I'm coughing, I'm short of breath, I can't get up from the couch,'" Siegel recounted. "The next day he was on hydroxychloroquine and antibiotics, per his cardiologist, he got up the next day, he was fine."
"This man is my father, Tucker," Siegel said.
"Wow," Carlson responded. "That couldn't be a clearer and heavier example."
Study: Zinc, HCQ, Z-Pack Cocktail Effective Early Vs. COVID-19
https://www.newsmax.com/Health/health-news/zinc-hydroxychloroquine-azithromycin-covid-19/2020/06/24/id/974003/
Quote:
The key note of this preprinted study, according to CrowdProtocol doctors, is the early treatment of COVID-19 in outpatients before they require hospitalization for a severe COVID-19 case, the latter of which was used to suggest no benefit to HCQ use in hospitalized patients.
"What differentiates this study is that patients were diagnosed very early with COVID-19 in an outpatient setting and treated early on," co-author of the study, Alexion Pharma Germany Dr. Roland Derwand said in a statement provided to Newsmax. Dr. Derwand worked the study with Dr. Martin Scholz and Dr. Vladimir Zelenko of Lenox Hill Hospital in Monroe, N.Y.
"Unfortunately, we seem to have forgotten that it is common medical knowledge to treat any patient with a disease as soon as possible. Dr. Zelenko treated his patients immediately with the three drugs to increase effects and didn't wait for the disease to develop."
A news release of the study declares hospitalization of 141 high-risk patients who were treated was 84% less likely than the untreated group. Just one patient died in the treated group vs. 13 patients that died from the untreated group.
"At this point, the media has left us with a grim view of anything related to hydroxychloroquine, but that is why studies like this are so important," Dr. Zelenko said in a statement.
Preliminary Injunction Sought to Release Hydroxychloroquine to the Public
https://aapsonline.org/preliminary-injunction-sought-to-release-hydroxychloroquine-to-the-public/
IMHO, this chart tells a big story...
Quote:
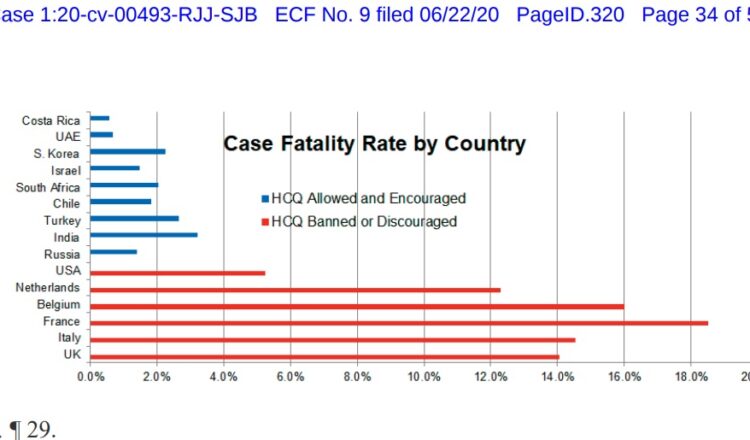
Quote:
Today the Association of American Physicians & Surgeons filed its motion for a preliminary injunction to compel release to the public of hydroxychloroquine by the Food & Drug Administration (FDA) and the Department of Health & Human Services (HHS), in AAPS v. HHS, No. 1:20-cv-00493-RJJ-SJB (W.D. Mich.). Nearly 100 million doses of hydroxychloroquine (HCQ) were donated to these agencies, and yet they have not released virtually any of it to the public.
Featured Stories
See All
CHAMPS! Aggie women's tennis claims second national championship
by Richard Zane
41:12
5h ago
2.6k
Weaver's second masterpiece puts A&M in rarefied air
by Richard Zane
Baseball Thoughts: Personifying 'rough, tough, real stuff'
by Ryan Brauninger
Aggie baseball places six on All-SEC teams
by Richard Zane